
Making the right choice when treating the edentulous maxilla
Given the increased acceptance and greater understanding of the benefits of dental implants, the author suggests guidelines for the treatment planning of the edentulous maxilla. Treatment of the resorbed, edentulous upper jaw with a fixed implant-supported prosthesis is subject to a set of maxilla-specific challenges.
For the surgeon, the presence of the bilateral maxillary sinuses places restrictions on the placement of implants in the posterior portion of the maxilla, where they may be needed to establish adequate anterior-posterior force distribution. For the restorative dentist, achieving adequate phonetics and stable masticatory function are essential considerations.
With edentulism comes alveolar atrophy
The edentulous alveolus undergoes both horizontal and vertical resorption in the absence of internal loading (Fig 3a & 3b). Healthy maintenance of the alveolar bone depends largely on internal loading from either tooth roots or dental implants. (Brånemark et al 1985). A fixed, implant-supported restoration provides the loading necessary to prevent alveolar atrophy.
When a fixed, implant-supported prosthesis is likely to be indicated, a systematic pretreatment approach for evaluating the edentulous patient is essential (Bedrossian 2008). This approach to treatment planning allows for better communication within the implant team as well as with the patient. The results? Predictable esthetic, phonetic and functional outcomes for the patient!
-
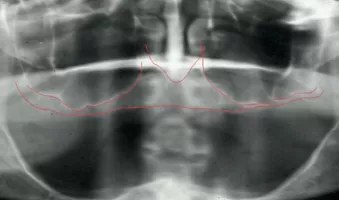
Maxillary sinuses limit the available bone for the posterior placement of implants
-
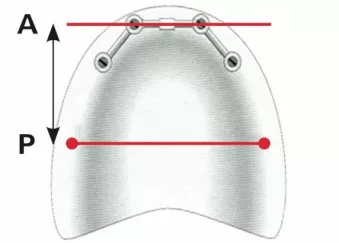
Anterior-Posterior distribution of the implants is limited by the maxillary sinus.
-
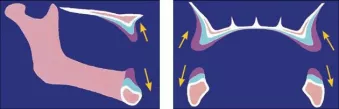
Depiction of the vertical, lingual and posterior resorption pattern of the maxilla.
-

No alveolar atrophy — the cervical portion of the denture teeth is adjacent to the gingival crest.
-

Composite defect — note the space between the crest of the denture teeth and the gingival crest.
-

Dentures removed, smiling, the maxillary crest is not displayed in this case.
-
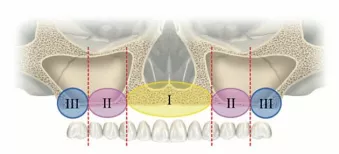
Zones of the maxilla. (See article for the key to use and subsequent images for illustrations).
-

Presence of bone in all three zones allows for the axial placement of implants.
-
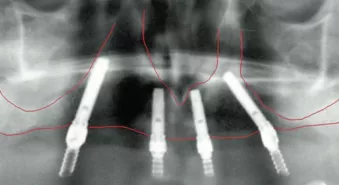
Presence of bone in zones I and II allows for treatment using the tilted implant concept.
-
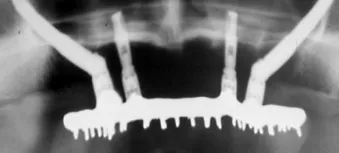
Presence of bone in zone I only, allows for treatment using the Zygoma concept.
-

Insufficient bone in all three zones, allows for treatment using the Quad-zygoma concept.











Systematic evaluation of the edentulous maxillae
Three factors considered early in the examination process can be key determinants for the successful fixed restoration treatment of the completely edentulous maxilla.
These factors are:
- The presence or absence of a composite defect,
- The position of the transition line, and
- The zone locations in the maxilla, as revealed in a panoramic survey.
Please note that the evaluation of these three factors is not intended to be a substitute for thorough diagnosis and the development of a treatment plan (Bedrossian 2006).
The presence or absence of a composite defect
Comprehensive evaluation of the edentulous maxilla is further complicated by the fact that both bone and soft tissue loss can begin before tooth removal as a result of generalized periodontitis—which often causes the appearance of “long teeth.”
Edentulous patients may present with intact alveolar bone volume, missing only the clinical crowns. These patients are considered as tooth-only defect patients.
Patients who present with missing teeth as well as resorption of their alveolar bone and loss of soft tissues (Fig. 5) are considered to have a composite defect.
In order to create an esthetically pleasing final fixed prosthesis, differentiating between these two types of patients is essential. By duplicating the patient’s denture and evaluating the space between the cervical portion of the denture teeth and the crest of the soft tissues, a tooth-only defect and a composite defect can be readily identified. For patients who do not have a composite defect, a fixed porcelain-fused-to-metal (PFM) restoration may be considered. For patients who present with a composite defect, a NobelProcera Implant Bridge or a milled bar, implant-supported overdenture may be considered.
Visibility of the residual ridge crest
To evaluate the esthetics of the final restoration, the transition line (i.e. the line where the prosthesis ends and the soft tissues begin) should be evaluated preoperatively.
With the patient’s maxillary denture removed, the patient should be asked to smile (Fig. 6). If the soft tissue of the edentulous ridge cannot be seen, the transition between the planned implant-supported prosthesis and the residual soft tissue crest will not be visible, allowing for an esthetic outcome. For a patient with a composite defect whose transition line can be seen, however, alveolplasty at the time of implant surgery is indicated if a NobelProcera Implant Bridge is planned.
On the other hand, if the planned final prosthesis is a milled bar (implant-supported overdenture), there is no need for alveolplasty.
Zones of the maxilla
To determine whether axial implants, tilted implants or the zygoma implant concept should be considered, we divide the maxillary alveolus into three separate zones.
Zone 1 — cuspid to cuspid
Zone 2 — the premolar region
Zone 3 — the molar region
The presence or lack of adequate bone in each of the maxillary zones strongly affects the choice of surgical technique. To wit:
– If bone is adequate in all three zones, axial implants can be placed (Fig. 8).
– The tilted implant concept should be considered if only Zones I and II have adequate bone (Fig. 9).
– If only Zone I has adequate bone, the zygomatic treatment concept should be considered (Fig. 10).
– In the rare cases where all three zones lack adequate bone, the quad zygoma treatment concept can be considered (Fig. 11).
Presence of bone: Surgical approach
Zone I, II, III = Traditional (axial)
Zone I, II = All-on-4® treatment concept
Zone I only = Zygomatic implants
Insufficient bone = Quad zygoma